PMEL 17 / gp100 / Melanosome (MSVA-617R)
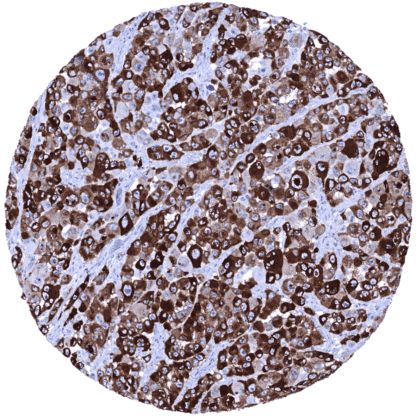
Recombinant Rabbit monoclonal / IgG 1:50 – 1:100 Research Use Only Cytoplasmic Human MSVA-617R 95kDa melanocyte-specific secreted glycoprotein, M-beta, Melanocyte lineage specific antigen GP100, Melanocyte protein Pmel 17, Melanoma associated ME20 antigen, Melanosomal matrix protein17, p100, p26, PMEL17, Premelanosome protein, Secreted melanoma-associated ME20 antigen, SILV, Silver homolog Skin: A moderate to strong cytoplasmic PMEL immunostaining should be seen in all melanocytes of the skin. Colon: PMEL immunostaining should be completely absent in all cells. PMEL 17 is expressed in normal and neoplastic melanocytes. Premelanosome protein (PMEL), also termed gp100 is a 100 kDa glycoprotein that is encoded by the PMEL gene at 12q13.2 . PMEL is a pigment cell-specific protein responsible for the formation of fibrillar sheets within the pigment organelle, termed melanosome. The fibrillar sheets function as a template upon which melanins polymerize as they are synthesized. The PMEL fibrils are needed for optimal pigment cell function, as animals that either lack PMEL protein or express deficient (mutant) PMEL variants show varying extents of hypopigmentation and pigment cell impairment. The expression of the PMEL gene is regulated by the microphthalmia-associated transcription factor (MITF). The PMEL protein is a therapeutic target used in melanoma patients for vaccination and other treatment modalities. Among normal adult tissues a cytoplasmic PMEL immunostaining is seen in melanocytes of the skin. An additional (faint) granular cytoplasmic PMEL immunostaining located immediately below the apical cell membrane can be seen in gallbladder epithelium. This is considered a tolerable antibody cross-reactivity. These findings are largely consistent with the RNA and protein data described in the Human Protein Atlas (Tissue expression PMEL) Positive control: Skin: A moderate to strong cytoplasmic PMEL immunostaining should be seen in all melanocytes of the skin. Negative control: Colon: PMEL immunostaining should be completely absent in all cells. PMEL immunostaining is absent in the colon mucosa. Strong PMEL immunostaining is seen in melanocytes of the skin. Kidney, cortex Normal tissue gallery A positive PMEL immunostaining is seen in the majority of malignant melanomas. In benign melanocytic naevus, the epidermal part may be strongly stained while the dermal part is weakly stained or negative. PMEL is also seen in most cases of blue naevus, cellular blue naevus, dysplastic naevus, and Spitz naevus. PMEL also occurs in various other neoplasms of melanocytic origin or differentiation, such as for example PEComas derived from modified smooth muscle cells in the tuberous sclerosis complex (angiomyolipoma, lymphangioleiomyoma(-tosis), pulmonary sugar tumor, cardiac rhabdomyoma). The TCGA findings on PMEL RNA expression in different tumor categories have been summarized in the Human Protein Atlas. Malignant melanoma showing strong PMEL immunostaining in tumor cells. PMEL negative basal cell carcinoma containing few PMEL positive (non-neoplastic) melanocytes. PMEL negative anaplastic carcinoma of the thyroid. Cancer tissue gallery No data available at the moment IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein. All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well. Manual protocol Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target ... PMEL is a promising therapeutic target used by various treatment modalities. Its therapeutic potential is still under investigation. PMEL expression is not detected in all malignant melanomas and the expression levels vary between individual tumors. The prognostic/clinical impact of PMEL expression levels is unclear in melanomas and should be investigated. There are two ways how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. comparison with a second independent method for target expression measurement across a large number of different tissue types (orthogonal strategy), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target (independent antibody strategy). Orthogonal validation: For the antibody MSVA- 617R , specificity is suggested by the strong concordance of its immunostaining data with data from three independent RNA screening studies, including the Human Protein Atlas (HPA) RNA-seq tissue dataset, the FANTOM5 project, and the Genotype-Tissue Expression (GTEx) project, which are all summarized in the Human Protein Atlas (Tissue expression PMEL) . Immunostaining by using MSVA- 617R was almost exclusively detected in the skin, for which PMEL ...