Progesterone Receptor (MSVA-570R)
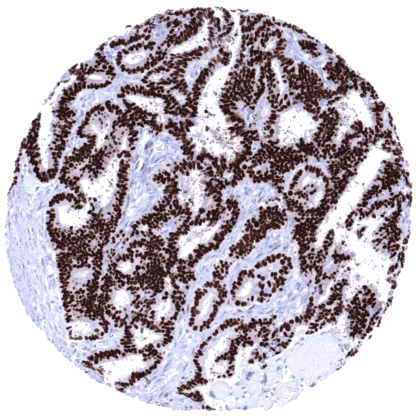
Recombinant Rabbit monoclonal / IgG 1:50 Research Use Only Nucleus Human MSVA-570R R3C3, Nuclear receptor subfamily 3 group C member 3, PGR, PR, PRA, PRB, Progesterone receptor form A, Progesterone receptor form B Uterine cervix: almost all columnar epithelial cells, basal squamous epithelial cells and most of the stromal cells must show a strong nuclear staining with only minimal cytoplasmic staining. Tonsil: PR immunostaining should be absent in all epithelial and non-epithelial cells. Progesterone Receptor is expressed in progesterone dependent cell types. The progesterone receptor (PR), is a nuclear receptor protein coded by the PGR gene residing on chromosome 11q22. It is activated by the steroid hormone progesterone. In the absence of progesterone its carboxyl terminal inhibits transcription of target genes. After binding to progesterone, a structural change of the PR protein terminates the inhibitory action, the protein dimerizes, enters the nucleus, binds to DNA and induces transcription of target genes. Progesterone antagonists prevent the structural reconfiguration. Progesterone and its receptor are key elements of female reproduction. In breast development, progesterone is involved in the formation of lobular-alveolar units. In human endometrium, progesterone directs glandular differentiation, stromal proliferation and development of decidual cells. PR shares considerable sequence homology with the estrogen receptor (ER) in the DNA-binding central domain. The presence of a functional ER is required for PR synthesis in the cell. ... Progesterone Receptor staining pattern in Normal Tissues with antibody MSVA-570R (images are shown in our “Normal Tissue Gallery”) Brain Cerebrum Negative. Cerebellum Negative. Endocrine Tissues Thyroid Negative. Parathyroid Negative. Adrenal gland Weak to moderate PR staining of a variable fraction of adrenocortical cells (not in all samples). Pituitary gland Weak to moderate PR staining of a variable number of epithelial cells in the adenohypophysis. Staining is absent in the neurohypophysis. Respiratory system Respiratory epithelium Negative. Lung Negative. Gastrointestinal Tract Salivary glands Weak to moderate PR positivity of some cells. Esophagus Weak to moderate PR positivity of some muscular cells in the muscular wall. Stomach Negative. Duodenum Weak to moderate PR positivity of some cells in Brunner glands. Small intestine Weak to moderate PR positivity of some muscular cells in the muscular wall. Appendix Negative. Colon Negative. Rectum Negative. Liver Negative. Gallbladder... The TCGA database on RNA expression in cancer has described the highest levels of PR expression in breast and endometrial cancer followed by ovarian and cervical cancer. Most other important tumor entities are described to be usually “PR negative”. The TCGA findings on Progesterone Receptor RNA expression in different tumor categories have been summarized in the Human Protein Atlas. Invasive breast cancer of no special type (NST) with strong PR immunostaining of tumor cells. Endometroid ovarian carcinoma with strong PR immunostaining of tumor cells. Endometroid endometrium carcinoma with strong PR immunostaining of tumor and stroma cells. Cancer tissue gallery Progesterone receptor (PR) (MSVA-570R) publication summary Relevant publication: Viehweger et al. “ Diagnostic and Prognostic Impact of Progesterone Receptor Immunohistochemistry: A Study Evaluating More Than 16,000 Tumors ”. Pathol (Amst). 2022 Aug 8;2022:6412148. PMID: 35992051 A total of 16,445 tumors were successfully analyzed from 147 different tumor categories by using the following protocol: Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH7,8 Target Retrieval Solution buffer. MSVA-570R at a dilution of 1:50 at 37°C for 60 minutes. Visualization of bound antibody by the EnVision Kit (Dako, Agilent). This protocol was also used for all stainings depicted in our tumor and normal tissue galleries. In this study, at least one progesterone receptor (PR) positive case was seen in 55 (37.4%) of 147 tumor categories and 31 (21%) tumor categories included at least one case with strong positivity. PR immunostaining was detected in 57.4% of breast tumors, 28.6% o... IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein. All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well. Manual protocol Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7,8 Target ... The diagnostic utility of PR expression analysis should be investigated in a large cohort of tumors from different entities. The clinical/biological significance of the rare ER-/PR+ breast cancers is unclear. Much is still unknown on the site-specific role of PR in various different tissues.