CD3 (MSVA-003R)
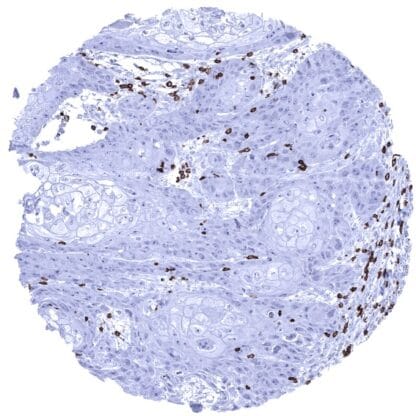
Recombinant Rabbit monoclonal / IgG 1:100 – 1:200 Research Use Only Cell surface. Cytoplasm. Human MSVA-003R CD3 epsilon; CD3 TCR complex; T cell antigen receptor complex epsilon subunit of T3; T-cell surface antigen T3/Leu-4 epsilon chain; T-cell surface glycoprotein CD3 epsilon chain; T3E; TCRE; TiT3 complex Tonsil: Amoderate to strong membranous staining should be seen in all T-cells in the interfollicular T-zones and in the germinal centres (few cells). Tonsil: All epithelial structures and B-cells should not show any CD3 immunostaining. CD3 is expressed on T-lymphocytes. CD3 (cluster of differentiation 3; OKT3) is a protein complex containing four distinct chains that jointly act as a T cell co-receptor. It is involved in activating both cytotoxic T cells (CD8+ naive T cells) and T helper cells (CD4+ naive T cells). The CD3 protein complex associates with the T-cell receptor (TCR) and the zeta-chain to form the TCR complex which generates an activation signal in T lymphocytes. CD3 is initially expressed in the cytoplasm of pro-thymocytes, the stem cells from which T-lymphocytes arise in the thymus. When the pro-thymocytes differentiate into common thymocytes, and subsequently into medullary thymocytes, the CD3 antigen begins to migrate to the cell membrane. CD3 is then found at the membranes of all mature T-cells. CD3 is a drug target for antibody-based treatment of acute graft rejection after transplantation. For cancer therapy, bispecific antibodies using anti-CD3 in combination with cancer surface proteins such as B7-H3 are being explored. CD3 immunostaining is only seen in T-cells. These predominantly occur in lymphatic organs such as thymus, lymph nodes and tonsils but are regularly also seen – at lower density – in many other tissue types. These findings are largely consistent with the RNA and protein data described in the Human Protein Atlas (Tissue expression CD3) Positive control = Tonsil: A moderate to strong membranous staining should be seen in all T-cells in the interfollicular T-zones and in the germinal centres (few cells). Negative control = Tonsil: All epithelial structures and B-cells should not show any CD3 immunostaining. Ileum, mucosa – In the ileum mucosa, CD3 positive T-lymphocytes are usually numerous Tonsil, surface epithelium – CD3 positive T-lymphocytes predominate in the interfollicular zone of the tonsil while they are less numerous in germinal centres Uterus, endometrium (proliferation) – In the endometrium, CD3 positive T-lymphocytes are regularly seen Normal tissue gallery CD3 is retained in almost all T-cell lymphomas and leukemias. A variable number of CD3 positive tumor infiltrating lymphocytes regularly occur in virtually all other neoplasms. Of note, CD3 can rarely be also expressed in B-cell lymphoma. The TCGA findings on CD3 RNA expression in different tumor categories have been summarized in the Human Protein Atlas. Large cell anaplastic T-cell lymphoma showing a moderate to strong CD3 positivity of tumor cells. Invasive breast cancer of no special type (NST) infiltrated by a significant number of CD3 positive T-cells. Hodgkin’s lymphoma, mainly composed of CD3 positive lymphocytes. Interspersed Hodgkin and Reed-Sternberg cells are CD3 negative. Cancer tissue gallery No data available at the moment IHC users have different preferences on how the stains should look like. Some prefer high staining intensity of the target stain and even accept some background. Others favor absolute specificity and lighter target stains. Factors that invariably lead to more intense staining include higher concentration of the antibody and visualization tools, longer incubation time, higher temperature during incubation, higher temperature and longer duration of the heat induced epitope retrieval (slide pretreatment). The impact of the pH during slide pretreatment has variable effects and depends on the antibody and the target protein. All images and data shown here and in our image galleries are obtained by the manual protocol described below. Other protocols resulting in equivalent staining are described as well. Manual protocol Freshly cut sections should be used (less than 10 days between cutting and staining). Heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 9 Target Re... The clinical significance of the number of intratumoral CD3 positive lymphocytes is under intensive research. CD3 is a key component of multicolor assays analyzing the role of lymphocyte subsets in cancers and other diseases. The prevalence of a positive CD3 immunostaining in hematological and non-hematological neoplasms should be further evaluated. There are two ways, how the specificity of antibodies can be documented for immunohistochemistry on formalin fixed tissues. These are: 1. Comparison with a second independent method for measuring target expression across a large number of different tissue types ( orthogonal strategy ), and 2. Comparison with one or several independent antibodies for the same target and showing that all positive staining results are also seen with other antibodies for the same target ( independent antibody strategy ). As a standard orthogonal validation process for MSVA antibodies, RNA data summarized in the Human Protein Atlas (Tissue expression CD3) are used for comparison. However, this procedure has limited validity for proteins that are expressed in significant subsets of lymphocytes because these cells occur in virtually all organs. The preferential CD3 RNA expression in the thymus and other lymphatic tissues such as the tonsil and lymph nodes fits with the staining pattern observed by MSVA-003R i...